

Introduction: Outcomes for acute myeloid leukemia (AML) among older patients has remained largely unchanged for decades. Long-term survival for patients aged >60 years is poor (median survival 10.5 months). Targeting the proteasome in AML is attractive, since leukemia stem cells have demonstrated sensitivity to proteasome inhibition in preclinical models, perhaps through down regulation of nuclear NF-KB (Guzman, Blood 2001). AML cell lines are susceptible to synergistic cytotoxicity when bortezomib, a proteasome inhibitor, is combined with daunorubicin and cytarabine. We have shown that adding bortezomib to standard treatment in AML results in a high remission rate, although grade 2 sensory neurotoxicity was noted in approximately 12% of treated patients. A newer generation proteasome inhibitor, ixazomib, is less frequently associated with neurotoxicity, and, therefore, was selected for combination with conventional chemotherapy in this phase I trial. The primary objective of this study was to determine the maximum tolerated dose (MTD) of ixazomib in combination with conventional induction and consolidation chemotherapy for AML. Herein are the initial results of this trial.
Methods: Adults >60 years of age with newly diagnosed AML were screened for eligibility. Patients with secondary AML were eligible, including those with prior hypomethylating agent therapy for myelodysplastic syndromes (MDS). We excluded those with promyelocytic leukemia. There were 2 phases in this study. In the first phase (A), the induction treatment consisted of the following: cytarabine 100 mg/m2/day by continuous IV infusion, Days 1-7; daunorubicin 60 mg/m2/day IV, Days 1, 2, 3, and ixazomib was provided orally at the cohort dose, Days 2, 5, 9, and 12. Consolidaton or transplant was at the discretion of the treating physician in phase A. In the second phase (B), induction was the same as that with the determined MTD of ixazomib. All patients were to be treated with the following consolidation: cytarabine at 2 g/m2/day, days 1-5 with ixazomib on days 2, 5, 9, and 12 at the cohort dose for consolidation.
A standard 3 + 3 patient cohort dose escalation design was used to determine whether the dose of ixazomib could be safely escalated in 3 cohorts (1.5 mg/day, 2.3 mg/day, 3.0 mg/day), initially in induction (phase A) and subsequently in consolidation (phase B). The determined MTD of ixazomib in the first portion (A) of the trial was used during induction in the second portion (B), which sought to determine the MTD for ixazomib during consolidation. Secondary objectives included rate of complete remission, disease-free survival, and overall survival (OS).
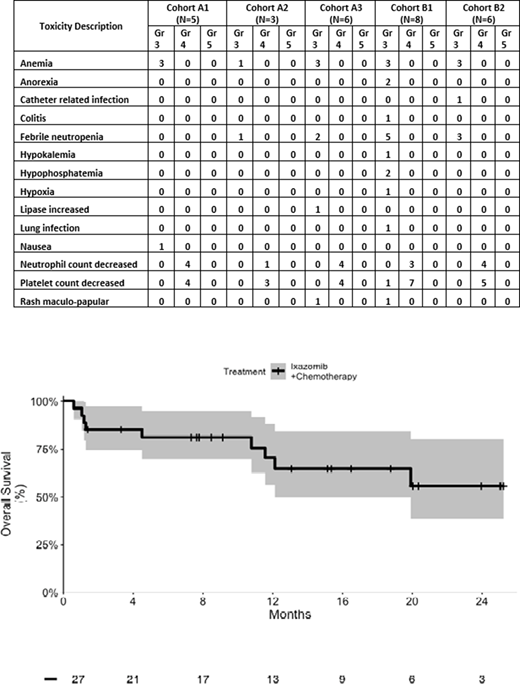
Results: Thirty-six patients have been enrolled on study, and 28 have completed dose levels A-1 through A-3 and B1 through B-2. Full information on cohort B-3 has not yet been obtained, hence, this report covers the experience with the initial 28 patients, cohorts A-1 through B-2. There were 12 (43%) patients among the 28 with secondary AML, either with prior hematologic malignancy or therapy-related AML. Nineteen patients (68%) were male, and the median age was 68 years (range 61-80 years). There have been no grade 5 toxicities due to study drug. Three patients died early due to leukemia, 2 of which were replaced for assessment of the MTD. Nearly all the grade 3 and 4 toxicities were hematologic (Table). There was 1 DLT (grade 4 platelet count decrease extending beyond Day 42). There has been no grade 3 or 4 neurotoxicity with ixazomib to date. Among the 28 patients in the first 5 cohorts, 22 achieved complete remissions (CR) and 2 achieved CRi, for a composite remission rate (CCR) of 86%. Among the 12 patients with secondary AML 8 achieved CR and 2 achieved CRi, for a CCR of 83%. The median OS for the 28 patients has not been reached (graph). The 18-month OS estimate was 65% [90% CI, 50-85%].
Conclusions: The highest dose level (3 mg) of ixazomib planned for induction in this trial has been reached safely. For consolidation there have been no serious safety issues in the first 2 cohorts with a dose up to 2.3 mg, apart from 1 DLT in the form of delayed platelet count recovery. The recommended phase 2 dose of ixazomib for induction is 3 mg. Accrual to cohort B-3 is ongoing. Notably, to date, no grade 3 or 4 neurotoxicity has been encountered. The remission rate in this older adult population with the addition of ixazomib to standard chemotherapy appears favorable.
Amrein:Amgen: Research Funding; AstraZeneca: Consultancy, Research Funding; Takeda: Research Funding. Attar:Aprea Therapeutics: Current Employment. Brunner:Jazz Pharmaceuticals: Membership on an entity's Board of Directors or advisory committees; Forty-Seven Inc: Membership on an entity's Board of Directors or advisory committees; AstraZeneca: Research Funding; Takeda: Research Funding; Celgene: Membership on an entity's Board of Directors or advisory committees, Research Funding; Novartis: Research Funding. Hobbs:Constellation: Honoraria, Research Funding; Novartis: Honoraria; Incyte: Research Funding; Merck: Research Funding; Bayer: Research Funding; Jazz: Honoraria; Celgene/BMS: Honoraria. Neuberg:Celgene: Research Funding; Madrigak Pharmaceuticals: Current equity holder in publicly-traded company; Pharmacyclics: Research Funding. Fathi:Blueprint: Consultancy; Boston Biomedical: Consultancy; BMS/Celgene: Consultancy, Research Funding; Novartis: Consultancy; Kura Oncology: Consultancy; Trillium: Consultancy; Amgen: Consultancy; Seattle Genetics: Consultancy, Research Funding; Abbvie: Consultancy; Pfizer: Consultancy; Newlink Genetics: Consultancy; Forty Seven: Consultancy; Trovagene: Consultancy; Kite: Consultancy; Daiichi Sankyo: Consultancy; Astellas: Consultancy; Amphivena: Consultancy; PTC Therapeutics: Consultancy; Agios: Consultancy, Research Funding; Takeda: Consultancy, Research Funding; Jazz: Consultancy.
Ixazomib is FDA approved for multiple myeloma. We are using it in this trial for acute myeloid leukemia.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal